If you are having trouble logging in to your account, it may be a pop-up issue. Please use Chrome or Edge to login. Click here for more information.

This article was originally printed in the May/June 2026 issue of the California Veterinarian magazine.
Cancer care in veterinary medicine has advanced dramatically over the past two decades. We biopsy earlier, stage more accurately, and treat more effectively than ever before. Yet one of the most powerful tools we have to influence treatment tolerance, immune competence, and quality of life does not sit in the pharmacy—it sits in the bowl. From the moment a biopsy confirms a diagnosis, dietary planning should become an intentional part of the oncology conversation.
Cancer is not simply a localized disease; it is a systemic metabolic condition. Tumors alter host metabolism, increase inflammatory mediators, and shift how the body utilizes carbohydrates, fats, and proteins. Many veterinary patients experience progressive muscle loss, even when body weight appears stable. This phenomenon, often called cancer cachexia, is associated with decreased treatment tolerance, poorer wound healing, reduced immune competence, and shorter survival times.
Understanding these metabolic changes allows clinicians to move beyond generic feeding advice. Cancer patients often have increased protein turnover and altered glucose metabolism. Lean body mass preservation becomes a central goal. Adequate high-quality protein intake supports muscle maintenance, immune function, and tissue repair, particularly during chemotherapy or post-surgical recovery.
Energy density also matters. Many oncology patients experience intermittent hyporexia due to nausea, pain, or treatment-related side effects. Diets with moderate-to-higher fat content can provide caloric density in smaller meal volumes, helping maintain body weight when intake fluctuates.
Carbohydrate restriction is a frequent topic raised by clients who have encountered the concept of “starving cancer.” While tumor cells preferentially utilize glucose, current veterinary evidence does not support extreme carbohydrate elimination as a proven therapeutic strategy. Clinicians should be prepared to discuss this topic with nuance, acknowledging metabolic theory while emphasizing evidence-based recommendations.
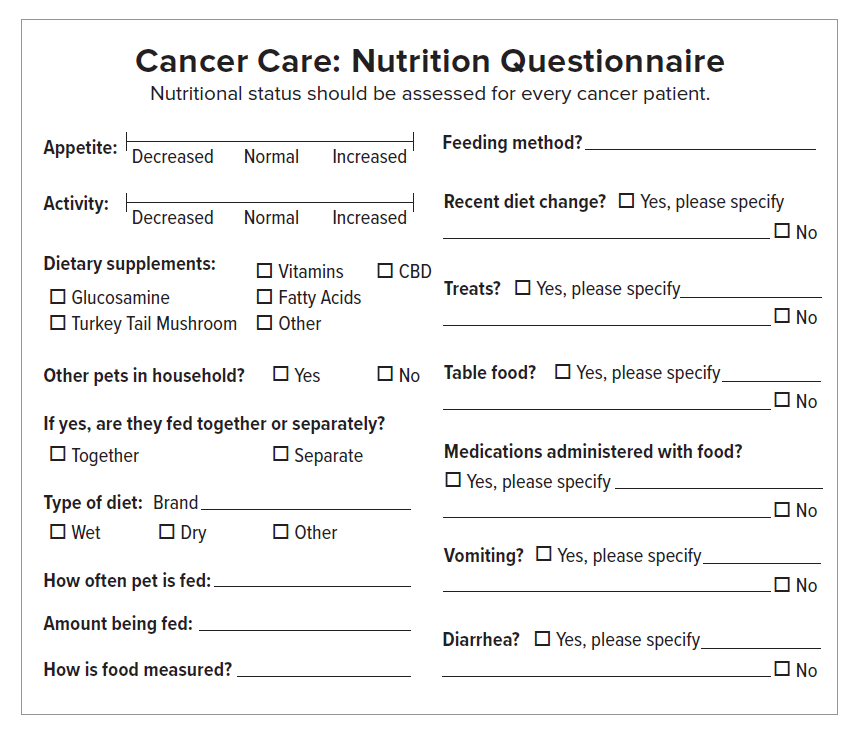
Routine nutritional assessment should be incorporated into every oncology visit. Body condition score and, importantly, muscle condition score should be documented at diagnosis and monitored regularly. Subtle epaxial muscle loss may precede weight decline and serve as an early warning sign for nutritional intervention. Caloric needs should be estimated and adjusted based on disease stage, treatment plan, and activity level.
Many patients do well on high-quality, balanced performance or recovery diets that meet increased protein and energy demands. For clients interested in home-prepared meals, referral to a board-certified veterinary nutritionist ensures dietary completeness and balance. Nutritional adequacy is especially critical in patients already compromised by systemic disease.
Treatment-related side effects frequently interfere with adequate intake. Chemotherapy and radiation can cause nausea, vomiting, diarrhea, mucositis, and food aversion. Proactive anti-nausea protocols and appropriate appetite stimulants can significantly improve consistency of intake. Adjustments in food texture, temperature, and palatability may help maintain interest in eating.
Feeding tubes are sometimes underutilized in oncology patients but can be transformative in select cases. Esophagostomy or gastrostomy tubes allow reliable caloric delivery, medication administration, and reduced mealtime stress. They are particularly valuable in feline patients, where even short periods of anorexia can precipitate hepatic lipidosis. Early consideration of assisted feeding often prevents crisis management later in the disease course.
Client communication is one of the most important components of nutritional oncology. Pet caregivers are frequently exposed to conflicting dietary advice, including raw feeding, boutique formulations, supplements, and various alternative regimens. Immunocompromised patients face increased risk from raw diets due to potential bacterial contamination, and supplement use may carry risks of drug interactions or unregulated dosing.
Rather than dismissing client research, clinicians should approach these discussions collaboratively. Acknowledging the emotional investment behind dietary decisions fosters trust. Clear, concise explanations of goals like maintaining muscle mass, supporting immune function, and preserving quality of life help anchor recommendations in shared priorities. Providing specific guidance reduces confusion and decreases the likelihood that owners will turn to unreliable sources.
Quality of life remains central to veterinary oncology. Nutritional goals may evolve over time. In early-stage or curative-intent cases, preserving lean mass and optimizing treatment tolerance are primary objectives. In advanced or palliative settings, flexibility may become more important than strict dietary structure. If a favored food maintains intake and enjoyment without compromising safety, that choice may align best with patient-centered care.
Importantly, once a patient develops one cancer, ongoing monitoring remains essential not only for recurrence or metastasis but also for nutritional status. Muscle loss can progress silently. Regular reassessment allows for timely adjustments and reinforces to clients that nutrition is a dynamic component of care, not a one-time recommendation.
Integrating nutrition into oncology case management elevates the standard of care. It requires intentional assessment, practical feeding strategies, proactive management of side effects, and confident client communication. While chemotherapy protocols and surgical margins often dominate discussion, the daily act of feeding exerts continuous influence on the patient’s metabolic state, strength, and comfort.
From biopsy to bowl, nutrition is not ancillary. It is therapeutic. By incorporating structured nutritional planning into cancer care, veterinarians can improve treatment tolerance, support immune health, and meaningfully enhance quality of life for dogs and cats facing a cancer diagnosis.
Dr. Kim Johnson is a board-certified veterinary oncologist, educator, and author dedicated to compassionate, purpose-driven medicine. Combining decades of oncology experience with a passion for mentoring and supporting the well-being of veterinary professionals, Dr. Johnson has delivered hundreds of hours of RACE-approved continuing education on cancer care, leadership, and resilience. She currently provides oncology consultations for Mission Pet Health.
Works Cited
Johnson, K. Assessing Nutritional Status of Cancer Patients. Hill’s Pet Nutrition. 2024.
Ruggiero C, Wakshlag JJ. Nutritional management of the canine and feline oncology patient. The Veterinary Clinics of North America: Small Animal Practice. 2022;52(6):1363-1381.
Ruggiero C, Michel KE. Cancer cachexia in veterinary patients: pathophysiology and clinical management. Journal of the American Animal Hospital Association. 2021;57(5):247-259.
Thamm DH, Vail DM. Nutritional considerations in veterinary oncology. In: Vail DM, Thamm DH, Liptak JM, eds. Withrow & MacEwen’s Small Animal Clinical Oncology. 6th ed. Elsevier; 2020:136-146.
Freeman LM, Becvarova I, Cave NJ, et al. World Small Animal Veterinary Association Nutritional Assessment Guidelines. Journal of Small Animal Practice. 2011;52(7):385-396.







