If you are having trouble logging in to your account, it may be a pop-up issue. Please use Chrome or Edge to login. Click here for more information.
If you are having trouble logging in to your account, it may be a pop-up issue. Please use Chrome or Edge to login. Click here for more information.

This article was originally printed in the Mar/Apr 2026 issue of the California Veterinarian magazine.
Corneal ulcers represent one of the most common ocular abnormalities presenting to the general practitioner. It is useful to think about ulcers in two broad categories: complicated and uncomplicated. Under the umbrella of complicated corneal ulcers is a specific type of ulcer called a Spontaneous Chronic Corneal Epithelial Defect (SCCED), sometimes also referred to as an indolent ulcer or Boxer ulcer. Like all ulcers, SCCEDs are painful and can be frustrating to treat, especially because they are frequently misdiagnosed at initial presentation as a routine, uncomplicated corneal ulcer. Unfortunately, client frustration with many weeks of treatment and failure of their dog’s eye to heal often leads to loss of the established clientveterinarian relationship and revenue.
In my experience, when a superficial corneal ulcer hasn’t healed in the normal expected time of a week, the general practitioner changes topical antibiotic. Many of these cases present to my referral hospital with a history of topical triple antibiotic therapy, followed by Terramycin, then Gentamicin or Ofloxacin, all of which represent poor antimicrobial stewardship. It also demonstrates failure in the basic understanding that topical antimicrobial treatment for a non-infected ulcer, such as a classic SCCED ulcer, does nothing to promote corneal wound healing but rather is implemented to prevent secondary infection.
To that end, a useful reminder when faced with any corneal ulcer is: “If an ulcer hasn’t healed in 7-10 days, change your diagnosis, not your antibiotic.” Reasons for which ulcers do not heal are as follows: 1) the underlying problem is still present (e.g. dry eye disease, entropion, ectopic cilia); 2) the ulcer is now infected (and thus by definition, “complicated”); or 3) the ulcer is a SCCED.
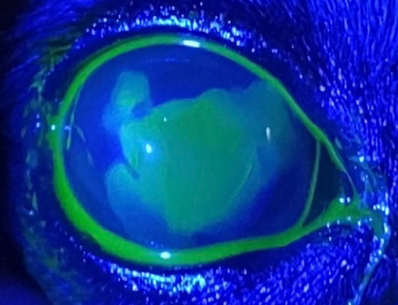
SCCED ulcers typically impact middle-to-older aged dogs, with Boxers, Boston Terriers, and French Bulldogs most commonly affected. SCCEDs are characterized by a redundant, loose lip of corneal epithelium (Figure 1), which often leads to a “halo” effect surrounding the ulcer bed on fluorescein stain (Figure 2) (figures courtesy of Dr. Taryn Overton). The reason SCCED ulcers fail to heal with conventional ulcer management is due to a defect in the cornea’s anterior stroma (an acellular hyalinized zone forms), preventing the overlying epithelium from adhering as it should. Thus, the key to appropriate management of this specific type of ulcer is early, correct diagnosis and correct intervention to promote healing.
As veterinary ophthalmologists, we are increasingly cognizant of qualitative—not just quantitative—tear film abnormalities.
Treatment Options
Because SCCEDs do not heal with standard medical therapy alone, the veterinarian must—at a minimum—manually remove all loose, non-adherent epithelium to “restart” the healing process. This is done after sterile prep with dilute betadine solution, adequate topical anesthetic, and light systemic sedation if needed. I strongly recommend dilating the pupil with 2-3 drops of atropine (1 drop 4-5 minutes apart) to help counteract the reflex uveitis that occurs with every ulcer, but will be made worse with your therapeutic interventions.

Treatment
At a minimum, using 8-10 dry, sterile cotton tip applicators (CTA), vigorously debride the redundant lip of epithelium and ulcer bed. The moment the Q-tip becomes “wet” with tears, use a dry one to ensure that all loose epithelium is adequately removed and the ulcer bed is slightly roughened. Wet CTAs do not have appropriate purchase ability. Approximately 50% of SCCEDs will heal using this treatment alone. After dry Q-tip debridement, to improve the chances of ulcer healing, a Diamond Burr Debridement (DBD) can be performed using a handheld, diamond-tipped motorized burr to gently polish the ulcerated surface after the loose epithelial cells are removed, helping the new epithelial cells anchor to the underlying stroma. This has a higher success rate (approximately 80–90%) after a single treatment. Another adjunctive therapy commonly performed after CTA debridement is grid or punctate keratotomy, whereby a 27-25 gauge needle is used to make tiny scratches or punctures in the cornea to promote epithelial adhesion. It is critical that these fine scratches cover the ulcer bed and go “clear cornea to clear cornea.”
Post SCCED healing procedure, patients should wear a hard Elizabethan collar to prevent self-trauma for two weeks until recheck examination. I typically treat my patients with QID topical antibiotics, oral trazodone, oral NSAID (e.g., Rimadyl or meloxicam), and gabapentin for sedation and pain relief. Sometimes, insertion of a bandage contact lens or collagen shield is also used. Finally, I urge practitioners to always check tear production in the contralateral eye, as keratoconjunctivitis sicca is far too commonly underdiagnosed and frequently an important underlying cause of recurrent SCCEDs. Additionally, for any patient I treat for a SCCED, I prescribe preservative-free lubricant at least twice daily to both eyes for life.
As veterinary ophthalmologists, we are increasingly cognizant of qualitative—not just quantitative—tear film abnormalities. Given the propensity of these ulcers to occur in our brachycephalic dogs, all dogs with this facial conformation, in my opinion, benefit from topical lubricant therapy starting at a young age and continuing throughout life. For this reason, I prefer using preservative-free eyedrops, which are readily available over the counter and from a variety of veterinary distributors and cannot harm the ocular surface.
Dr. Elizabeth Giuliano is a tenured professor of the Department of Veterinary Medicine and Surgery at the University of Missouri and the section chief of their comparative ophthalmology service. She has authored over 100 articles and textbook chapters. Dr. Giuliano is a dynamic, engaging speaker who has lectured extensively in the academic setting and at national and international meetings. She is the recipient of numerous teaching and leadership awards, including three Golden Aesculapius Teaching Awards, the Gold Chalk Award, the Dadd Award, Western Veterinary Conference’s 2018 “Educator of the Year,” and the 2023 Jordan Hoyt Memorial Tribute to Women faculty award. She served as the American College of Veterinary Ophthalmologists President from 2015–2016.

It’s Not About Politics….It’s About Your Profession. The CVMA-PAC is a bipartisan political action committee whose purpose is to educate state legislators and candidates on issues of importance to the veterinary profession






